

Across the United States, Community Health Centers (CHCs) have become the primary delivery system for pediatric care, especially among the nation’s populations with limited access to health care. They serve nearly 10 million children annually, about 1 in every 7 in the country. This is not a peripheral role in the health system – it represents a central responsibility for delivering cost-effective primary care and preventive health services to children at high risk for complex health conditions.
CHCs’ role becomes clearer when insurance coverage is considered. In 2024, more than 70% of children receiving care at CHCs relied on Medicaid, and another 12% were uninsured. This stands in sharp contrast to the overall CHC patient population, where about half depend on Medicaid and 18% lack insurance. Across the broader US child population, just 37% of children under 19 were covered by Medicaid in 2024, and only 6% were uninsured. Overall, CHCs provide care to roughly one in four Medicaid-covered and one in four uninsured children nationwide, focusing resources on those most at risk of care gaps.
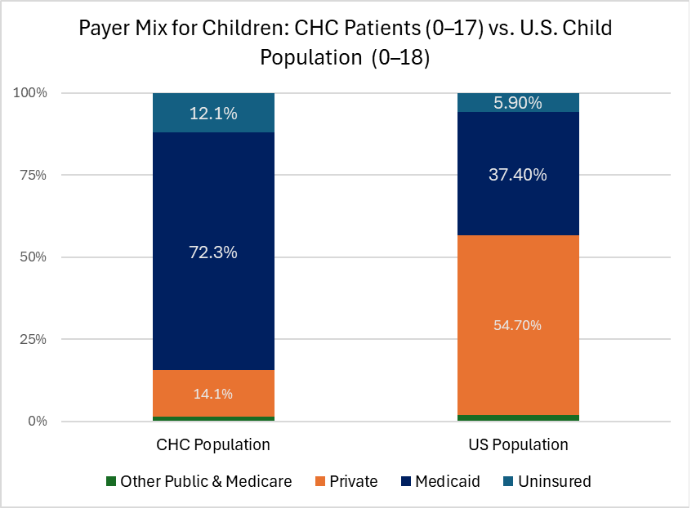
Data Sources: Bureau of Primary Health Care. (2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
Kaiser Family Foundation (KFF) State Health Facts. Children 0–18 with Health Insurance Coverage. Accessed from: https://www.kff.org/state-health-policy-data/state-indicator/children-0-18/
This is not incidental. Medicaid is now the dominant insurer for children, and CHCs have become its most important delivery platform. With significant Medicaid financing changes on the horizon, CHCs will face increased financial strain and administrative burden. The needs most directly affected include coverage continuity for children, payment stability for pediatric visits and developmental screenings, behavioral health integration, and care coordination. As coverage policies shift, CHCs will experience increased pressure as frontline providers for millions of families.
Children, Adolescents, and School-based Care
Children of all ages rely on CHCs, but some groups stand out. In 2024, nearly 4.4 million children seen at CHCs were ages 4-11, making them the largest pediatric age group served. These are the years when asthma, obesity, learning difficulties, and developmental delays are most often identified and addressed. Another 3.5 million adolescents received care at CHCs. Among adolescents, needs increasingly include behavioral health assessment, depression and anxiety screening, substance abuse screenings, and chronic disease management. Early identification and treatment during adolescence can substantially alter long-term health trajectories.
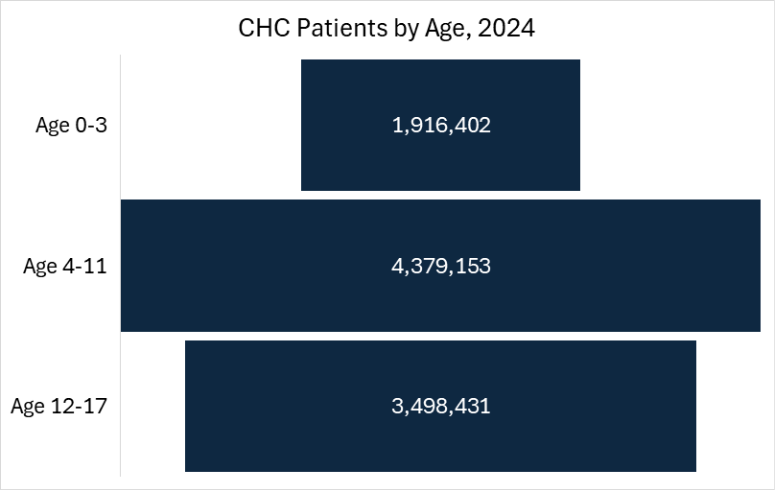
Data Source: Bureau of Primary Health Care. (2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
CHCs also operate more than 4,400 school‑based health centers (SBHC)—at least two‑thirds of all SBHCs nationwide—bringing care directly into the places where children spend much of their day. For Medicaid-covered and uninsured children, school-based sites are often the only reliable point of access to consistent care during the school year. These sites are especially important for families facing transportation barriers or limited access to pediatric specialists.
Taken together, these numbers show that CHCs are embedded in children’s everyday lives, managing chronic disease, identifying developmental needs, and supporting academic success through health.
The Workforce Behind Pediatric Care
To meet the needs of nearly 10 million young patients, CHCs rely on a comprehensive and dedicated workforce. In 2024, they employed more than:
- 3,400 pediatrician FTEs, who collectively provided over 10 million visits
- 7,600 family physicians, who delivered more than 19 million visits
- Thousands of nurse practitioners, physician assistants, behavioral health clinicians, and other essential providers
This blended workforce reflects the reality that in high-need communities, pediatric care is delivered through integrated primary care teams that must address medical, behavioral, and social complexities simultaneously. Within this care model, CHCs conducted 2.6 million childhood development screenings and evaluations for 1.8 million young patients. These screenings are the front line of early intervention, identifying speech delays, behavioral disorders, and chronic conditions before they become permanent barriers to learning and health.
Every one of those screenings reduces downstream costs in special education, emergency care, and disability services. However, delivery is dependent on stable staffing, adequate service payments, and the infrastructure to coordinate follow-up care.
Preventive Care on the Rise
Preventive care remains one of the core strengths of CHCs. In 2024, 67% of children ages 0–11 received a well‑child visit at a CHC—a rate that has increased even as workforce shortages and financial pressures have intensified. These visits are the foundation of pediatric medicine, which includes growth and development monitoring, behavioral health screening, and anticipatory guidance that shapes health for decades.
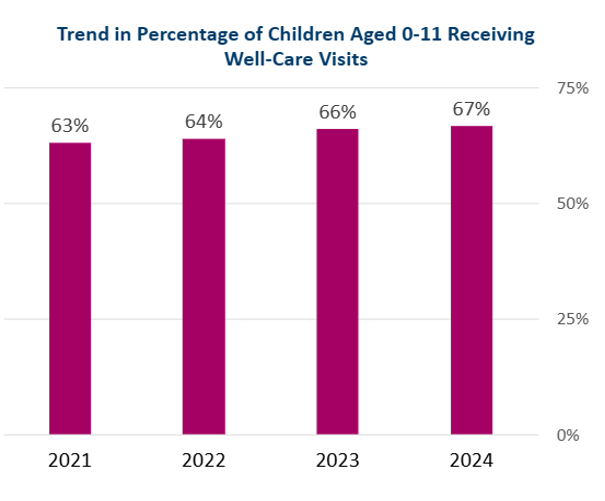
Data Source: Bureau of Primary Health Care. (2021–2024). Uniform Data System. Health Resources and Services Administration, U.S. Department of Health and Human Services.
When preventive care is consistent, children are healthier, schools are stronger, and communities face fewer avoidable medical and social costs. For Medicaid-covered and uninsured children, CHCs are often the only place where this continuity exists.
A Strategic Imperative
CHCs now operate as the nation’s largest primary care system for low-income children. The data is unequivocal: 1 in 7 of the pediatric population depends on CHCs for routine care, developmental screening, behavioral health, and early intervention. That means Medicaid and CHC policy, in practice, is pediatric policy. Changes in eligibility, payments, workforce support, or federal grant funding directly impact children’s access to reliable care and healthier long-term outcomes.
This also creates a new opportunity. With millions of children receiving continuous, community-based care, CHCs represent the most scalable platform in the country for improving early-life health and controlling long-term costs through prevention. Policymakers should recognize CHCs as the primary delivery system for pediatric care. Aligning Medicaid, workforce, and federal funding with that reality should be the defining task for child health policy.